A 30-year-old man has this for 1 year. You biopsy and find abundant mastocytes. What workup does he need? (CBC, tryptase level and bone marrow biopsy.)
A 30-year-old man has this for 1 year. You biopsy and find abundant mastocytes. What workup does he need? (CBC, tryptase level and bone marrow biopsy.)

You are seeing this 40 yow for routine follow up of her systemic mastocytosis. What are you looking for?
Patients should be examined periodically for any progression of disease, e.g., tumors, thickened areas, lymphadenopathy. The tryptase level should be followed. Ask about general health looking for any signs of systemic involvement, e.g. abdominal pain, diarrhea, nausea or vomiting, anemia or bleeding disorders, bone and muscle pain, enlarged liver, spleen or lymph nodes, depression, mood changes or problems concentrating.
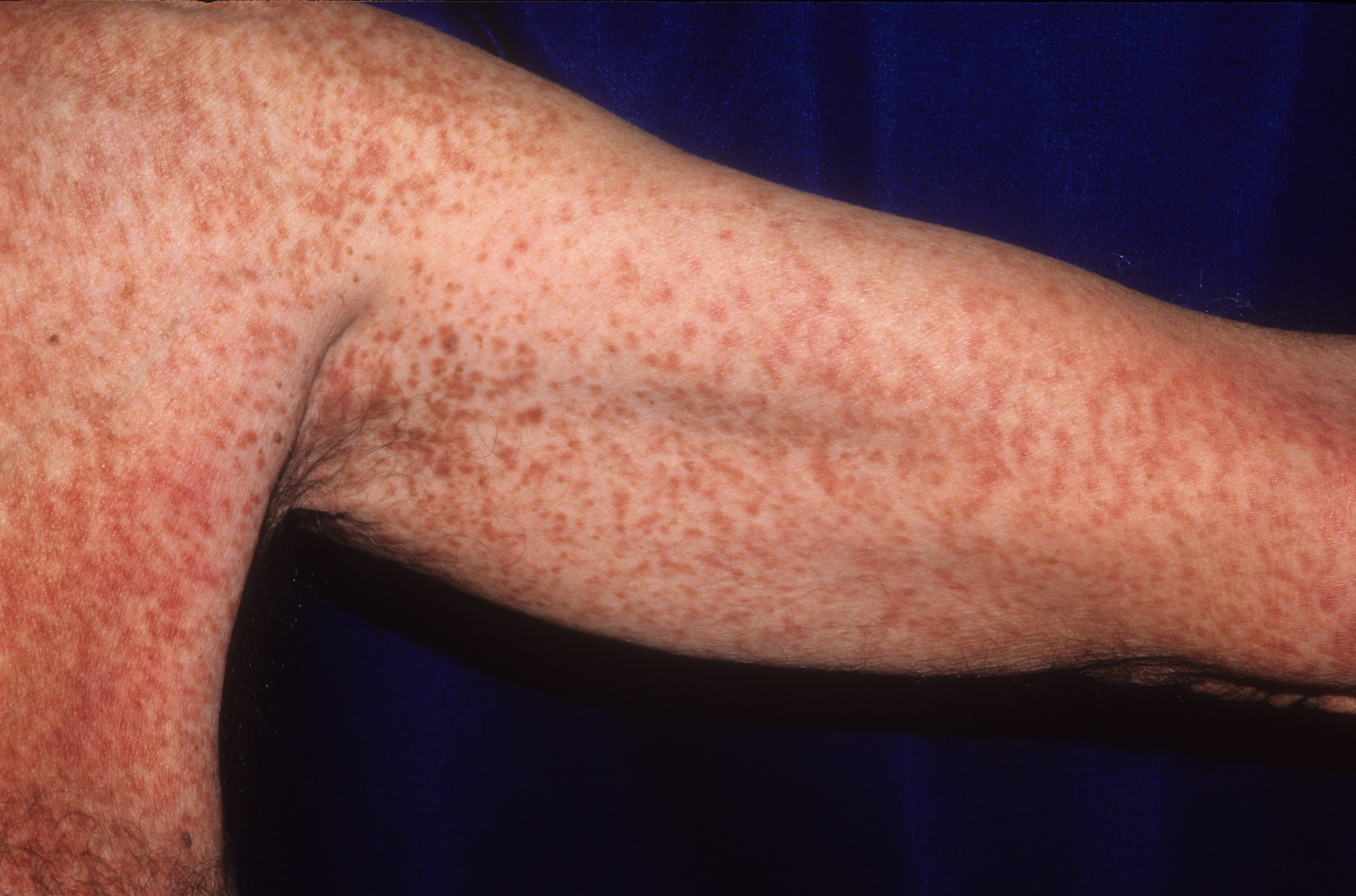
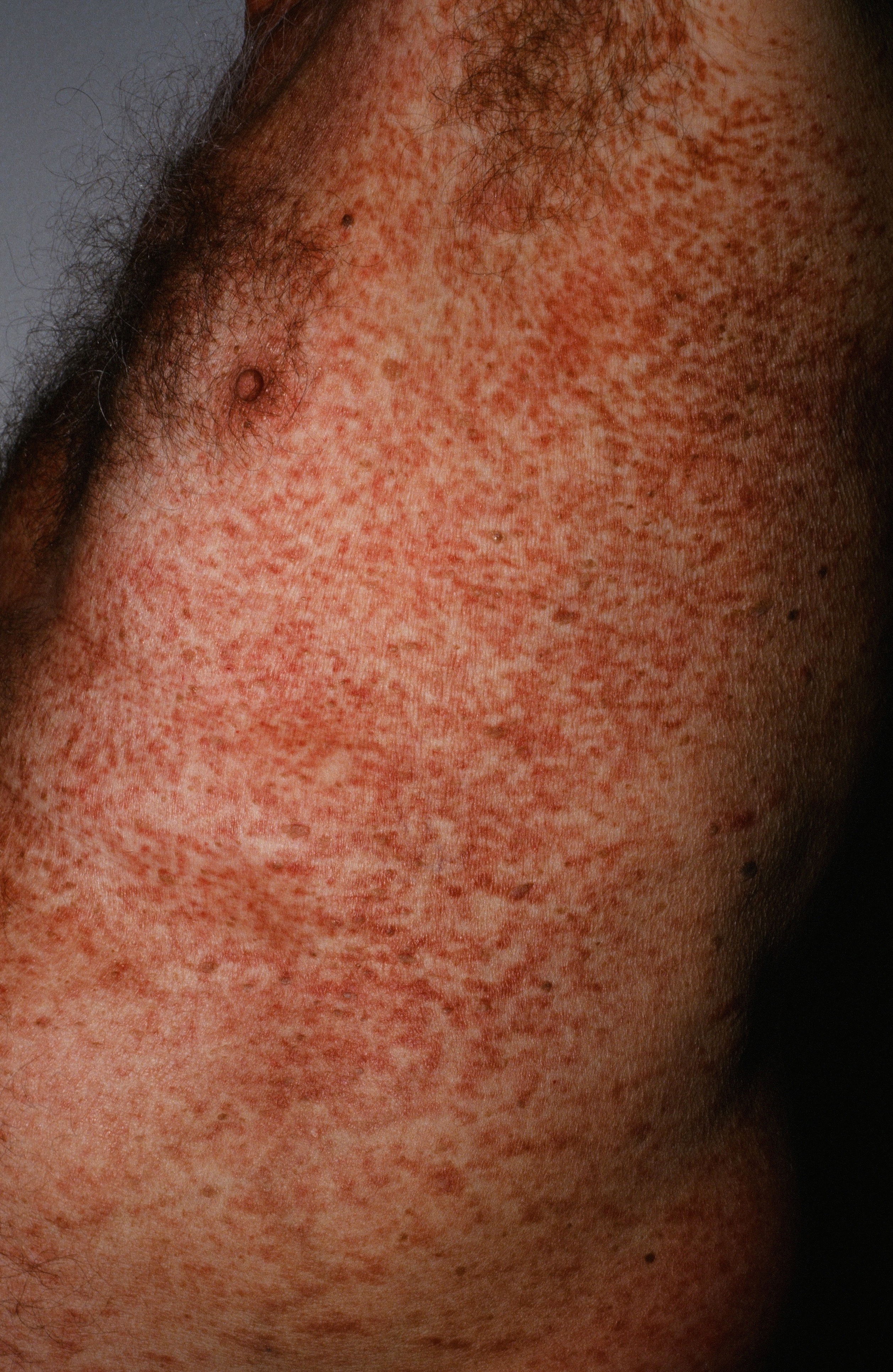
Systemic Mastocytosis (SM) is the abnormal proliferation of a clone of mast cells (MCs) that may invade the skin, bone marrow, and internal organs.
The skin may be infiltrated with mast cells causing red/brown papules and plaques. If severe, the skin can take on a thickened and doughy appearance. Both the infiltration of mast cells and their degranulation products can produce edema and a typical leather-grain appearance. Urticaria and flushing may be associated. Itch is common. Systemic symptoms may include abdominal pain, gastroesophageal reflux disease (GERD), and anaphylaxis. Physical findings can include hepatosplenomegaly and lymphadenopathy. In one study, 18% of patients with mastocytosis also had osteoporosis.
According to the 2008 World Health Organization, diagnosis is made by finding the one major criterion and one of the four minor criteria OR three of the four minor criteria.
A skin biopsy should be performed to establish the diagnosis. All patients should have a CBC with differential and a bone marrow biopsy. Measuring serum tryptase levels, serum histamine levels, and urinary histamine and its metabolites helps determine the systemic load of mast cells. Tryptase levels can be elevated by higher weight, impaired renal function, and increased age. For determining the need for a bone marrow biopsy in older, higher-weight patients, urinary methylimidazole acetic acid has a greater value than tryptase. The presence of KIT D816V mutation should be determined. A bone density test is appropriate since patients are at risk for osteoporosis and even bone fractures.
Homepage | FAQs | Use of Images | Contact Dr. White