
The classic butterfly rash of lupus. The ANA was positive (1:1320) as was the Ro antibody.
The classic butterfly rash of lupus. The ANA was positive (1:1320) as was the Ro antibody.
Cutaneous lupus (CLE) is an umbrella term for skin-only lupus. Discoid lupus (DLE) is the most common type of cutaneous lupus and it typified by redness, scaling, atrophy, hyperkeratois, and hyper and hypopigmentation. Other types of CLE include SCLE, acute lupus (e.g. butterfly rash), neonatal LE. The term DLE is often used in which skin lesions are found in a patient who does not satisfy the criteria for SLE.
Cutaneous lupus can take many forms. Erythematous, hypopigmented, atrophic, hyperkeratotic lesions scattered on the face are characteristic. The scale may fill the follicular orifices and if confluent, may be peeled back and the undersurface found to resemble the undersurface of a carpet (so-called carpet-tack sign). Sun exposure is a precipitating factor. The border may be hyperpigmented. Scarring can occur. Rarely, SCC may develop in chronic CLE lesions.
One prospective study of 77 patients with CLE found that 17% of patients eventually met the criteria for SLE. The mean duration between CLE and SLE was 8 years. Risk factors for progression included positive ANA, widespread discoid lesions, female sex and increased numbers of SLE criteria initially. It is thus recommended that patients get a CBC, ANA if applicable, urinalysis and ROS pertinent to the lupus criteria annually.

Discoid lupus (DLE) is the most common type of cutaneous lupus and it typified by redness, scaling, atrophy, hyperkeratois, and hyper and hypopigmentation.

A rash in the sun-exposed areas of a Black female should always bring up the consideration of lupus.

Hypertrophic Lupus Erythematosis (HLE) can mimic keratoacanthoma clinically and histologically, making it challenging to differentiate between the two. HLE, a variant of discoid lupus erythematosus, can present as verrucous plaques or keratoacanthoma-like nodules, especially on the face and arms.

Up to 45 percent of patients with SLE experience mouth sores.
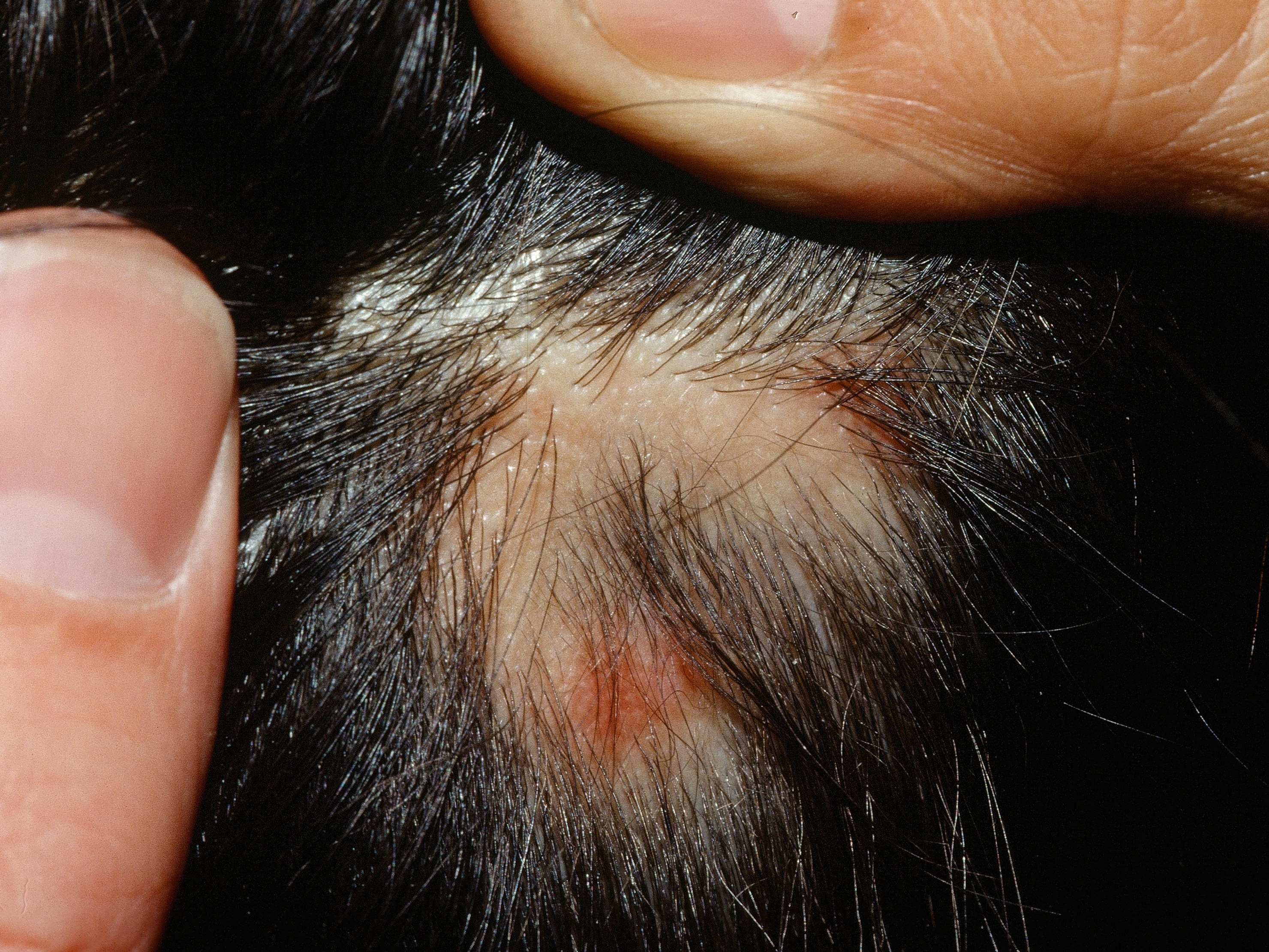
Lupus may cause diffuse, non-scarring alopecia, or focal, scarring alopecia as shown here.

A 10-year-old boy presents with this. Laboratory workup shows a positive ANA but no other abnormalities. Notably, complement levels were normal.
Homepage | Who is Dr. White? | Privacy Policy | FAQs | Use of Images | Contact Dr. White