
Periorbital edema with a violaceous hue is the classic heliotrope rash of dermatomyositis.
Periorbital edema with a violaceous hue is the classic heliotrope rash of dermatomyositis.
Dermatomyositis (DM) is a systemic disorder associated with characteristic skin changes (e.g., periorbital swelling, red papules on the knuckles) and symmetrical muscle weakness of the proximal limbs.
Periorbital edema with a violaceous hue is the classic heliotrope rash of dermatomyositis. A photodistributed eruption may be seen on the chest, upper back, and arms. Violaceous, scaly changes may occur over bony prominences, such as the knuckles, elbows, and scapula. Periungual erythema and telangiectasias occur. Hypertrichosis may occur rarely, especially in DM of childhood. The Jo-1 antibody correlates with pulmonary disease. Dermal collagen implants may pose a small but significant risk for the development of dermatomyositis. A dermatomyositis-like syndrome has been reported with acute HBsAg-positivity [JAMA 1978;239;959] and with hydroxyurea therapy [BJD 1995;133;455]. Scaling and fissures on the lateral and palmar aspects of the fingers may occur (mechanic's hands).
The term Gottron papules may be an outdated one, as it suggests a limited presentation. Skin changes over the knuckles may include papules, nodules, and plaques. The appearance may be erythematous, whitish (lichen-sclerosis-like), poikilodermatous, and even crusty with ulcerations.
Gingival telangiectasias has been reported as a relatively common occurrence in juvenile dermatomyositis. Other mucous membrane findings include edema, erosions, ulcers, and leukoplakia-like areas.
Mamy cases are misdiagnosed as lupus (photosensitivity and biopsy shows interface dermatitis).
The most common DM-associated medications were hydroxyurea (50 [30.3%]), immune checkpoint inhibitors (16.4%), statins (13.3%), penicillamine (6.1%), and tumor necrosis factor inhibitors (6.1%). Histopathologic testing, when undertaken, helped establish the diagnosis. There was a median time of 60 (21-288) days between drug initiation and drug-induced DM onset. History of cancer was reported in 85 cases (51.6%).
Hydroxyurea-induced MD-like eruption may be indistinguishable clinically from true DM, but it tends to be asymptomatic, characteristically lacks myositis, and is frequently associated with leg ulcers.
Scalp involvement may lead to significant alopecia. Patients are often misdiagnosed as having seborrheic dermatitis or psoriasis. There may be significant pruritus. It is often treatment-resistant. Treatment involves:
Note: not all of these antibodies are readily available and it is not clear as of this writing that their measurement is required for disease management.
A subset of patients with dermatomyositis have antibodies to MDA-5 (melanoma differentiation-associated gene 5). These patients are remarkable for normal ANA, palmoplantar or fingertip erythema, ulcerations (e.g., on the back of the hands), an increased risk of interstitial lung disease, mild or absent muscle inflammation and poor survival.
Proximal muscle weakness is the classic systemic sign. Patients may have trouble raising their arms above their head, rising from a chair, or squatting. Diagnosis may be aided by muscle enzyme elevation (check CPK, aldolase), muscle biopsy, and/or electromyography. MRI may be helpful in identifying muscle involvement and localizing it for biopsy. A subset of patients with skin disease but without muscle involvement (called amyopathic dermatomyositis) has been described. Lesions representing panniculitis may also occur in DM, both adult and juvenile. Various radiologic imaging studies have been recommended to localize muscle involvement. If needed, a radiologist should be consulted.
About 18-20% of DM patients do not have muscle involvement. About 3/4 of these patients are women. The diagnosis must be made clinically with the aid of skin histology as there is no muscle pathology to confirm. These patients still need a screen for malignancy and regular pulmonary function tests. Some of these patients will go on to develop muscle disease.
There is an approximate 20% incidence of cancer in adults but not for children under 16 years of age. Factors that increase risk for malignancy are: older age, severe skin disease, and ulceration. The risk for ovarian cancer is significantly higher in women. A search for an internal malignancy should be done, primarily through a thorough H&P and screening labs. Only very rarely has neoplasia (lymphoid tumors, neuroblastoma, and hepatocarcinoma) been associated with DM in children. The subset of patients with dermatomyositis sine myositis have a similar if not identical risk of neoplasia.
The types of malignancies found are broad and may include lung, colon, breast, hematologic, oropharyngeal, ovarian, renal, thyroid, esophogeal, prostate, thymic, melanoma, gastric, testicular etc.
Finally, ANA positivity is associated with malignancy. In one study of 231 patients with DM, 11% of ANA negative vs 43% of ANA positive patients developed a malignancy within 3 years.
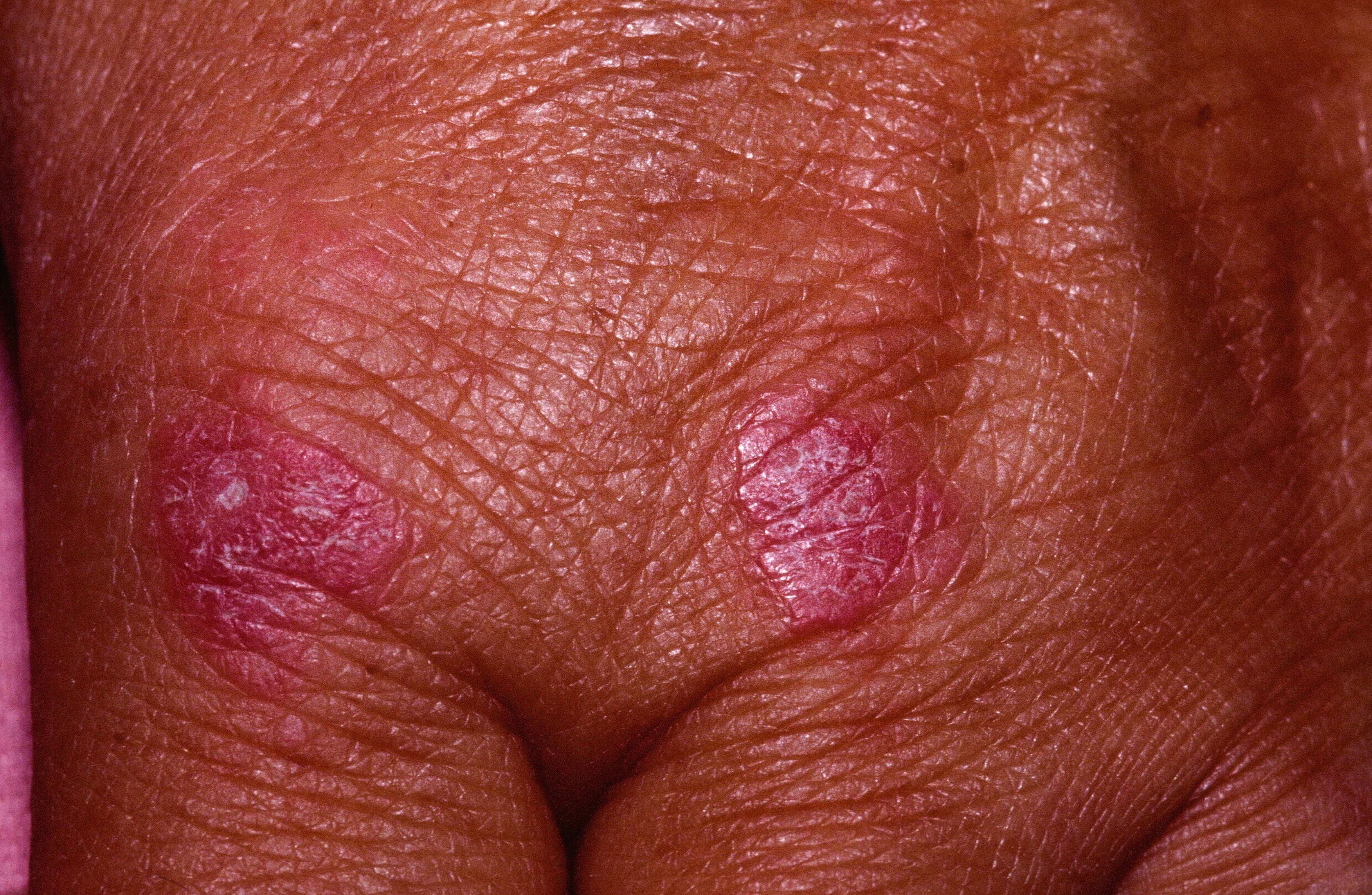 Violaceous plaques over the knuckles.
Violaceous plaques over the knuckles.

Periungual telangiectasias and erythema.
Homepage | Who is Dr. White? | Privacy Policy | FAQs | Use of Images | Contact Dr. White